
Nursing Notes Templates
A nursing note is read by the next nurse on shift, a physician, sometimes a lawyer, and it has to hold up for all of them. What it records, a change in condition, a treatment given, a patient’s response, becomes part of the clinical and legal record. These nursing notes templates follow the documentation methods nurses already use, so the structure is sound and your attention stays on recording the patient accurately. Pick the format your unit works in and start there.















A nursing note moves a patient’s story across the people caring for them. The nurse coming on shift, the physician reviewing progress, the team responding to a change all rely on what the previous note recorded, and how plainly it was recorded. Good nursing documentation is accurate, objective, and timed, and it records what happened and the patient’s response without leaving gaps a reader would have to fill in by guessing.
These nursing notes templates are built around the documentation methods nurses are trained in, so the format already prompts for what each kind of note needs. SOAP and SBAR structures keep an assessment or a handoff organized; admission, progress, and discharge formats follow a patient through an episode of care. The layout handles the order and the headings, which leaves your focus where it belongs, on observing the patient and recording it precisely. Charting accurately the first time is what keeps the record clear and the next clinician informed.
Worth knowing: In clinical documentation, the rule of thumb is that care which was not documented is treated as care that was not provided. Charting completely and on time protects the patient and the nurse alike, which is why a clear format that prompts for each element matters.
Kinds of nursing notes covered
The note formats here, and what each is used for.
Subjective, Objective, Assessment, Plan. A structured assessment format that keeps a clinical note consistent and easy for the team to read.
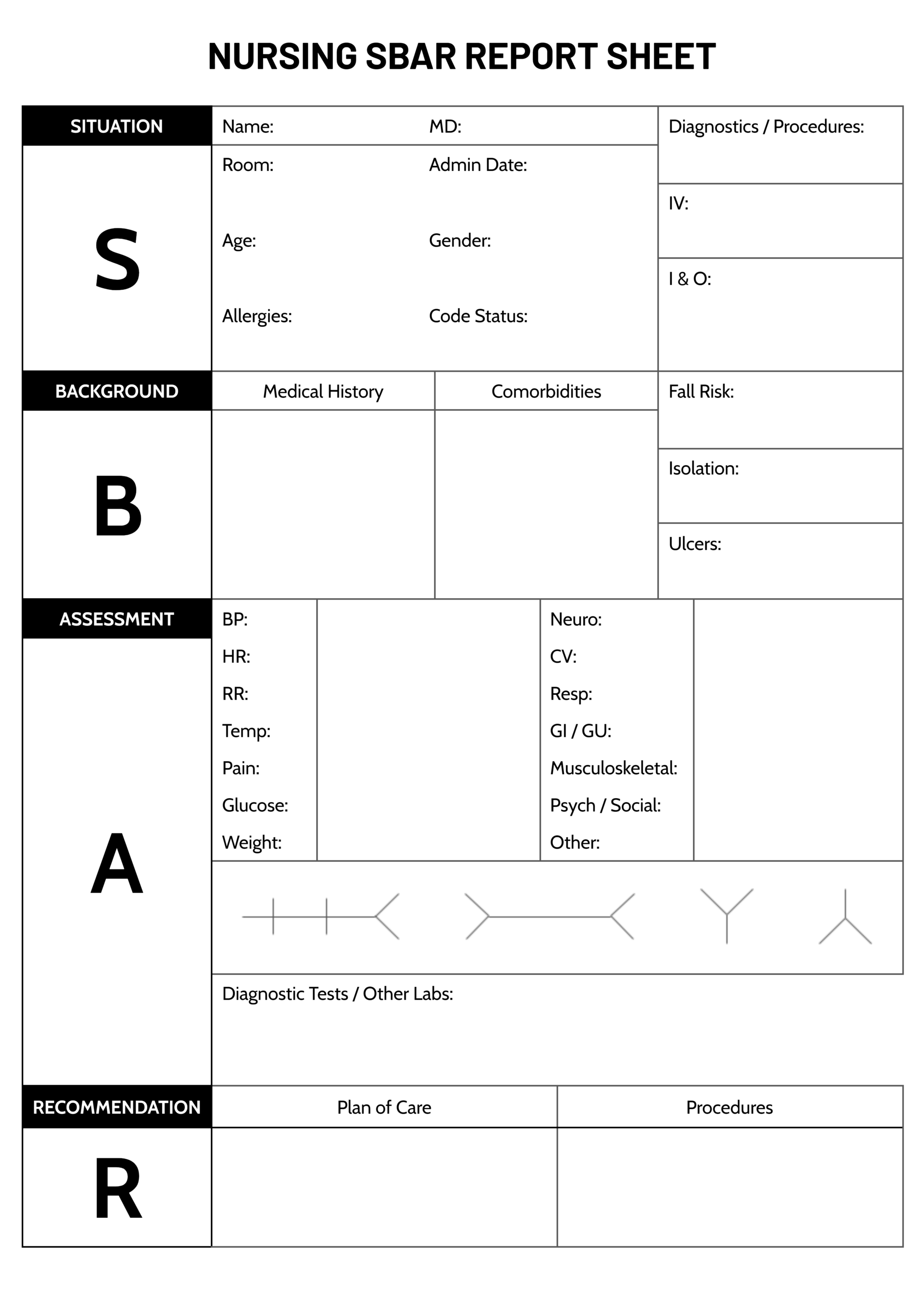
Situation, Background, Assessment, Recommendation. Built for clear handoffs and for escalating a concern to a physician quickly.
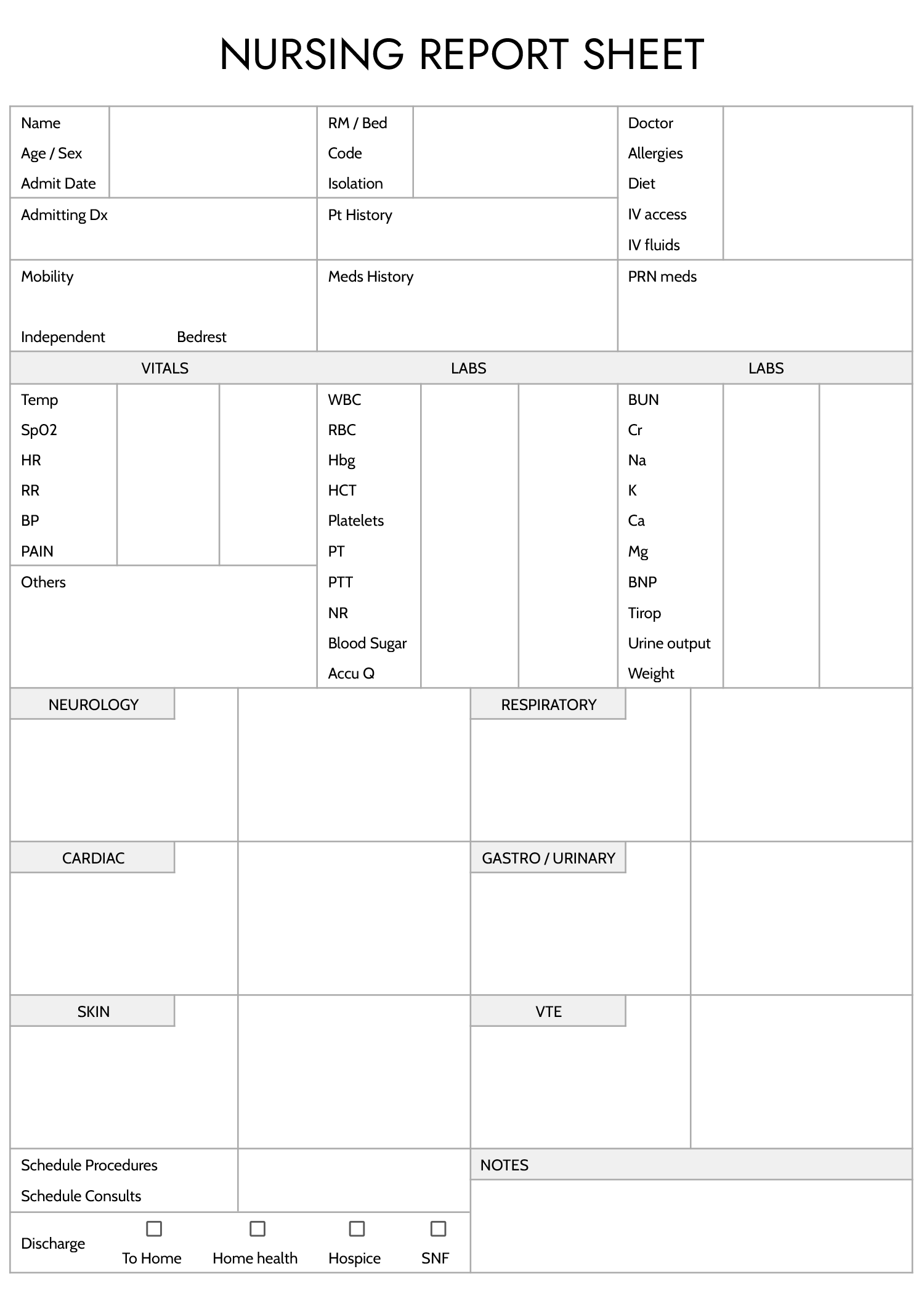
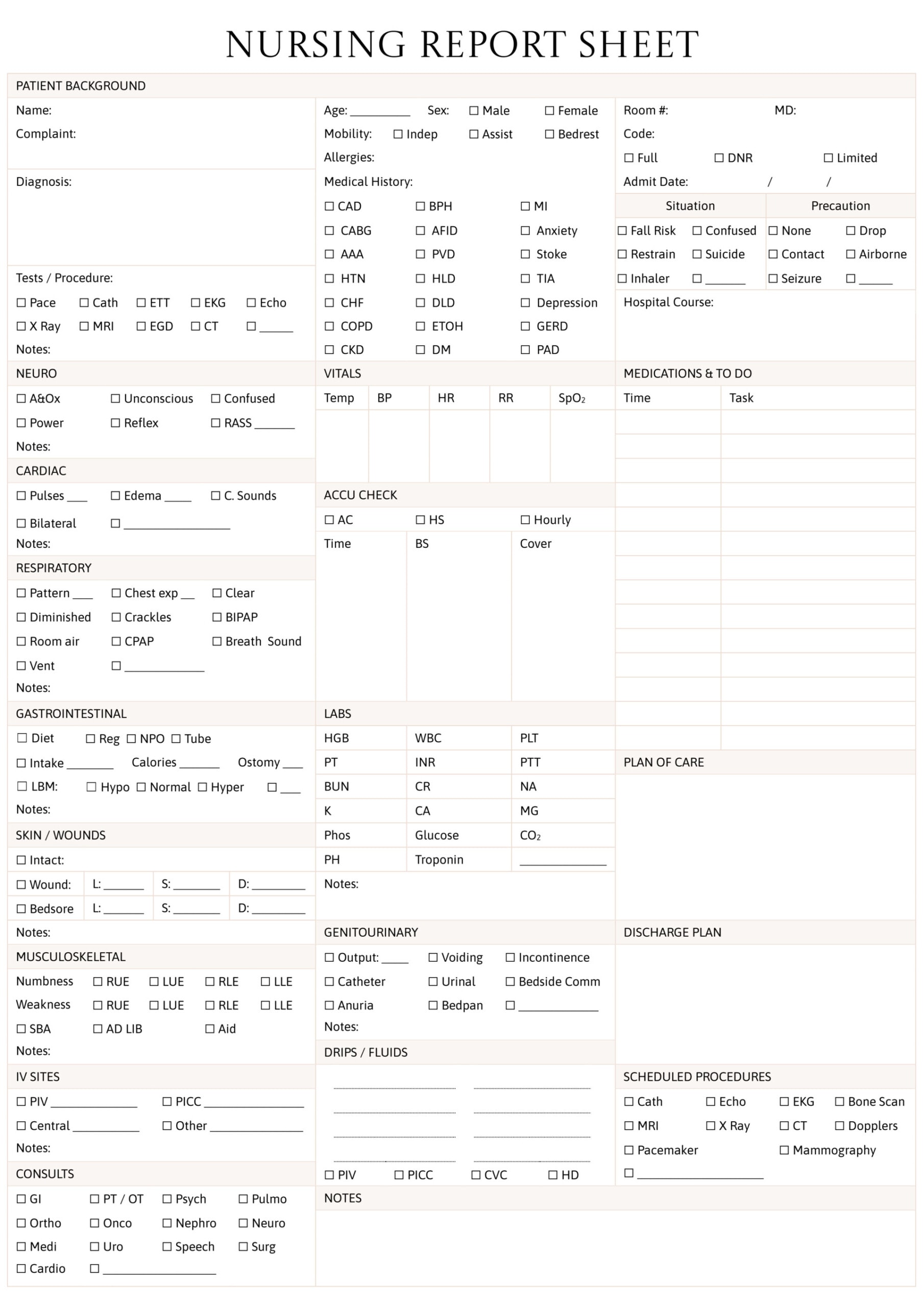
The baseline record taken when a patient is admitted, capturing history, status, and initial assessment for the team that follows.
Ongoing entries that track a patient's condition and response to treatment over a shift or a stay, so changes are visible.
The closing record of a patient's status, instructions, and follow-up at discharge, so care continues correctly after they leave.
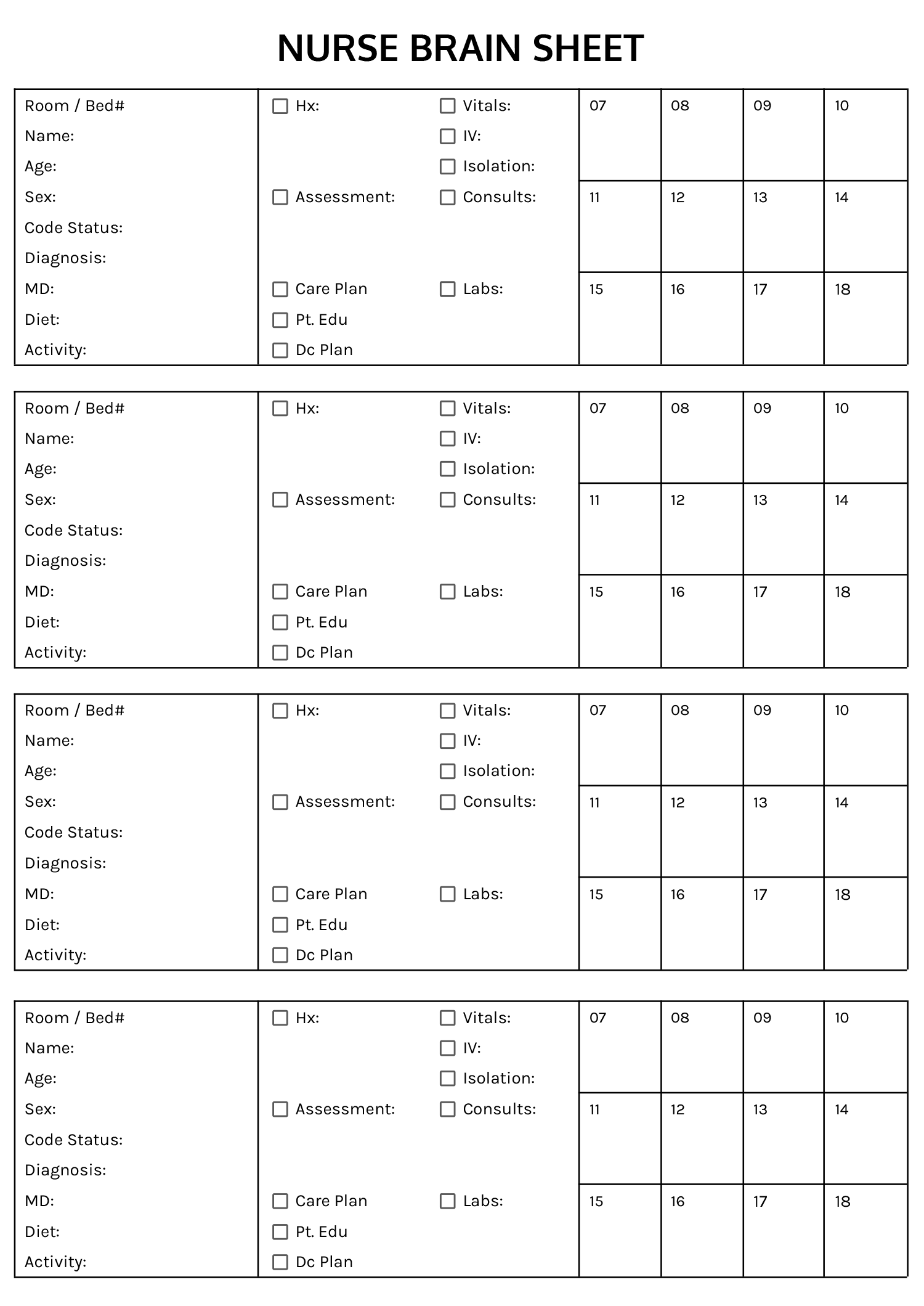
Nurse-to-nurse handoff sheets that organize a patient's key information so nothing essential is lost between shifts.
Writing a clear nursing note
What makes a note accurate, usable, and sound for the record.
Match the note to the moment, SOAP for an assessment, SBAR to hand off or escalate, an admission or discharge format at those points of care. The right format prompts for exactly what that note should contain.
Write what you observed and measured, vital signs, appearance, what the patient said, before your interpretation. Objective, specific entries are what make a note defensible and clear.
Record not just the intervention but how the patient responded to it, since the response is what the next clinician needs to judge what comes next.
Date, time, and sign each note. In a record where sequence matters clinically and legally, an unsigned or untimed entry loses much of its value.
Chart facts, not assumptions or opinion about the patient, and avoid leaving blanks that imply something was missed. A note is read later by people who must trust it exactly as written.
Hold an editable copy for your own use and keep the charted version intact as the record. Each template lists the formats shown on its card.
FAQs
What types of nursing notes do these templates cover?
The collection includes SOAP and SBAR formats, admission, progress, and discharge notes, and nurse-to-nurse shift report sheets. Each follows the structure that kind of note is expected to have, so you can pick the one your unit uses.
What is the difference between SOAP and SBAR?
SOAP (Subjective, Objective, Assessment, Plan) organizes a clinical assessment of a patient. SBAR (Situation, Background, Assessment, Recommendation) is built for communication, handing off a patient or escalating a concern to a physician fast and in order. Many nurses use both, for different purposes.
What should be avoided when writing a nursing note?
Avoid subjective opinion about the patient, vague wording, and recording an interpretation as if it were an observation. Late, unsigned, or untimed entries weaken the record, and blank fields can read as care that was missed. The aim is an accurate, objective, timed account of what happened and how the patient responded.
Can I adapt these templates to my facility's charting?
Yes. The headings and fields are editable, so you can align a template with your facility’s documentation standards and terminology. The format gives you the recognized structure as a starting point rather than a fixed form.