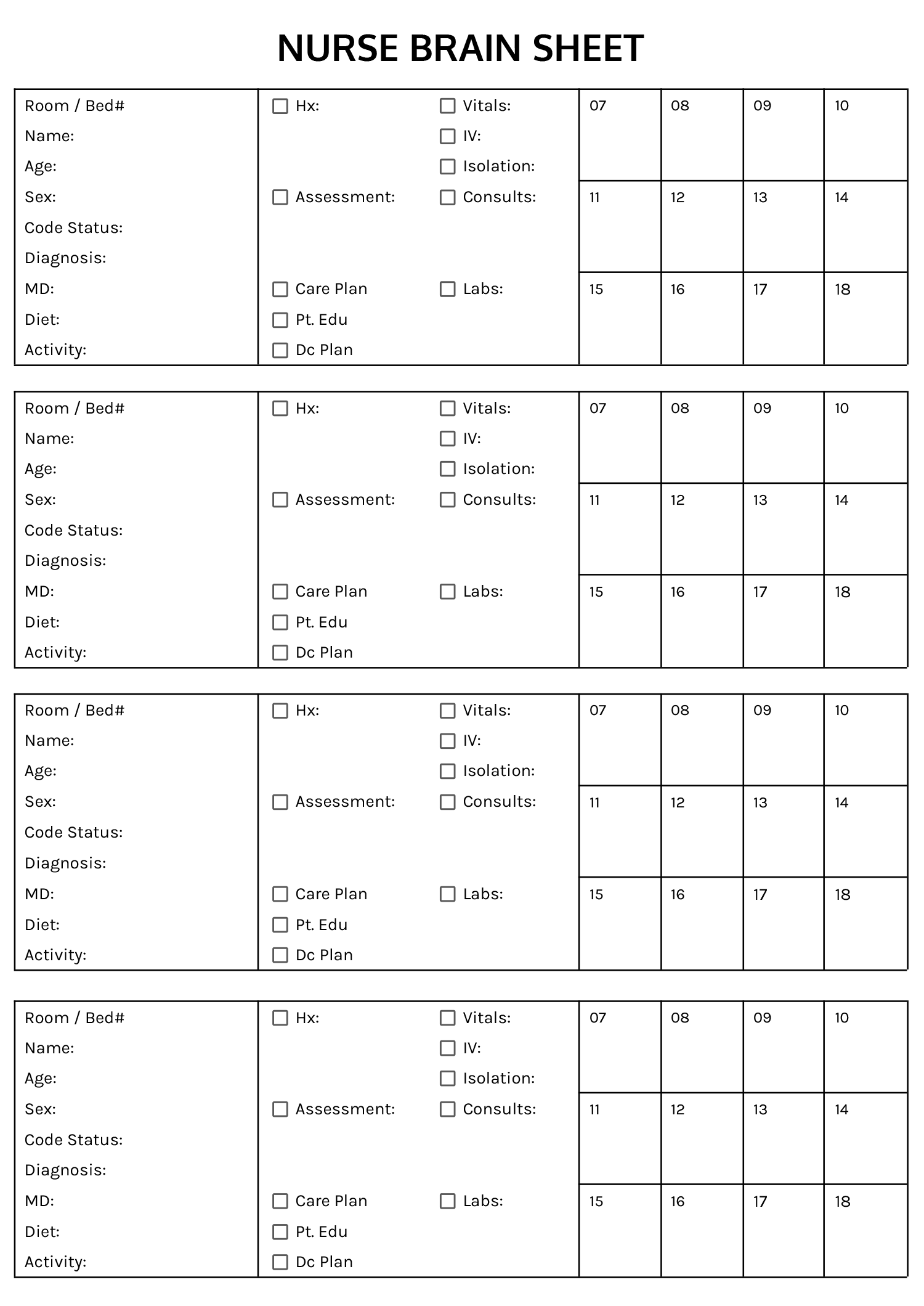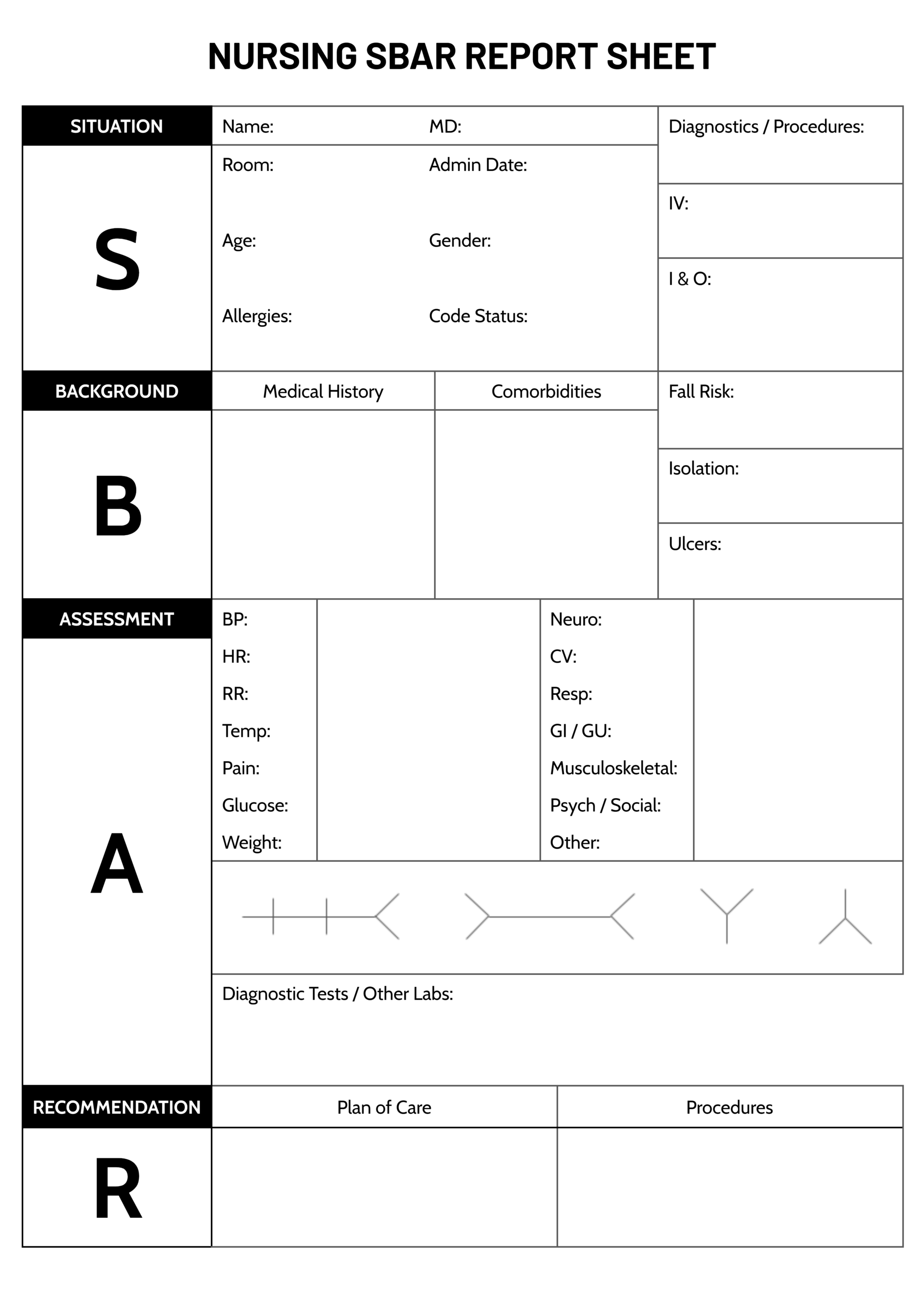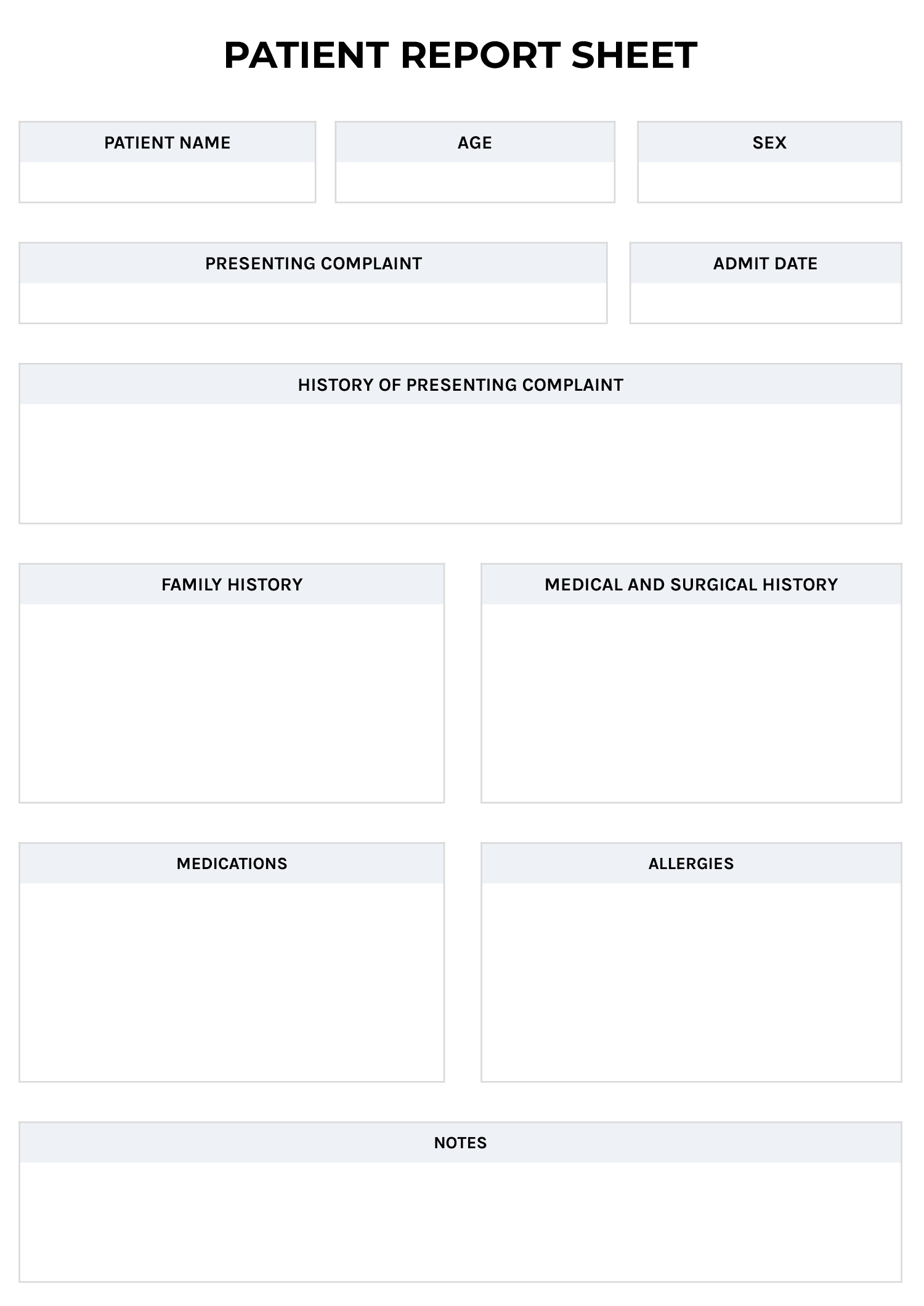


A nursing report sheet—also known as a nursing brain sheet—is used to document key patient information throughout a nurse’s shift and maintain continuity of care during handoffs or patient transfers. It stays with the nurse for quick reference during rounds and is updated in real time so the incoming shift can quickly understand the patient’s condition and the planned care or interventions.
The report sheet includes sections for personal details, diagnosis, vitals, and current care activities. Filling each section thoroughly is essential to ensure important patient information is easily accessible not just for nurses during shift changes but also for doctors and other healthcare providers when the patient is transferred to another unit such as the ICU, emergency department, or a specialty ward.
How to Use This Report Sheet
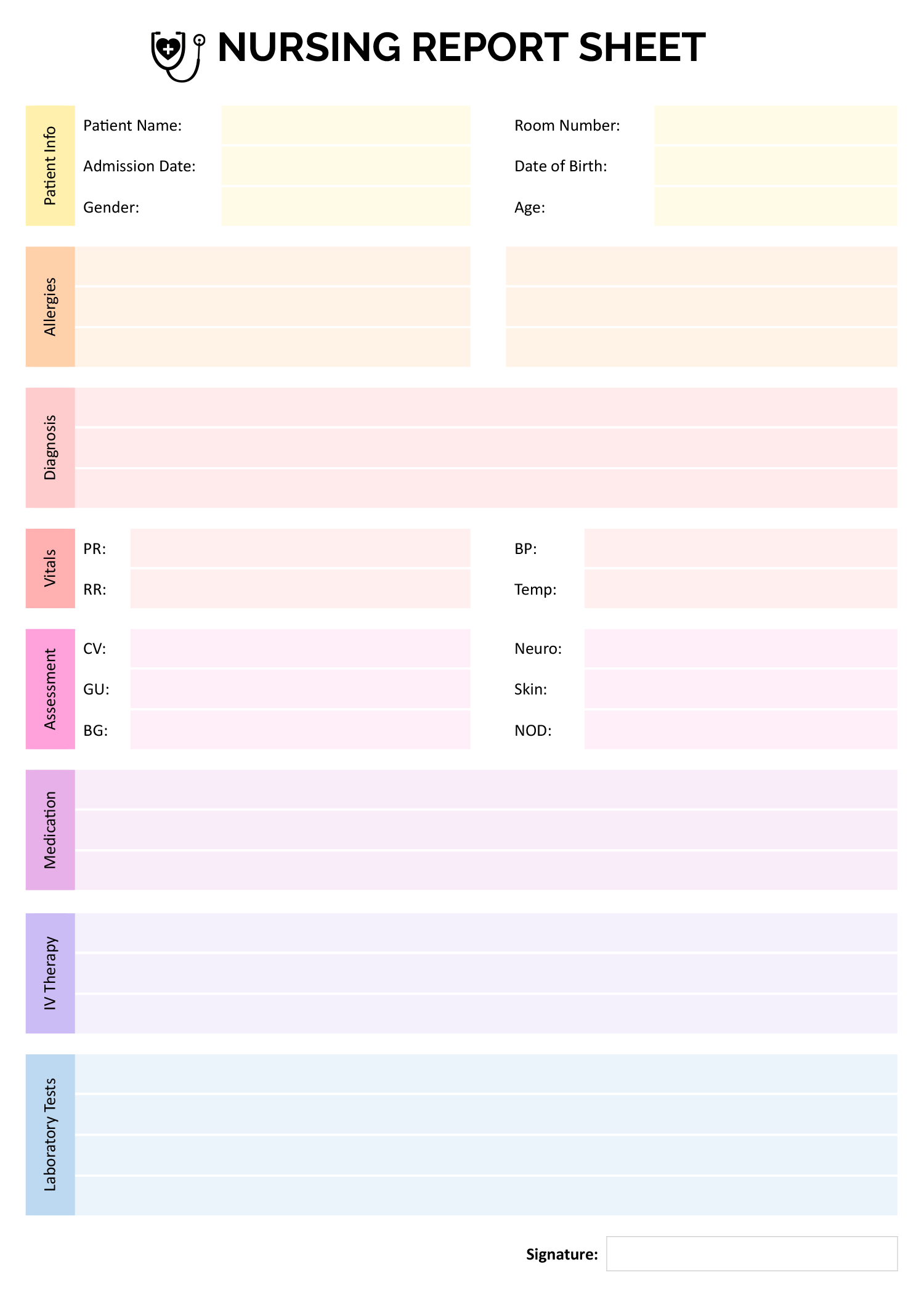
This nursing report sheet is available in both Microsoft Word and Google Docs formats. Each section of the nursing report sheet designed to capture specific clinical and patient care information. This guide explains each field for accurate documentation and safe patient transitions.
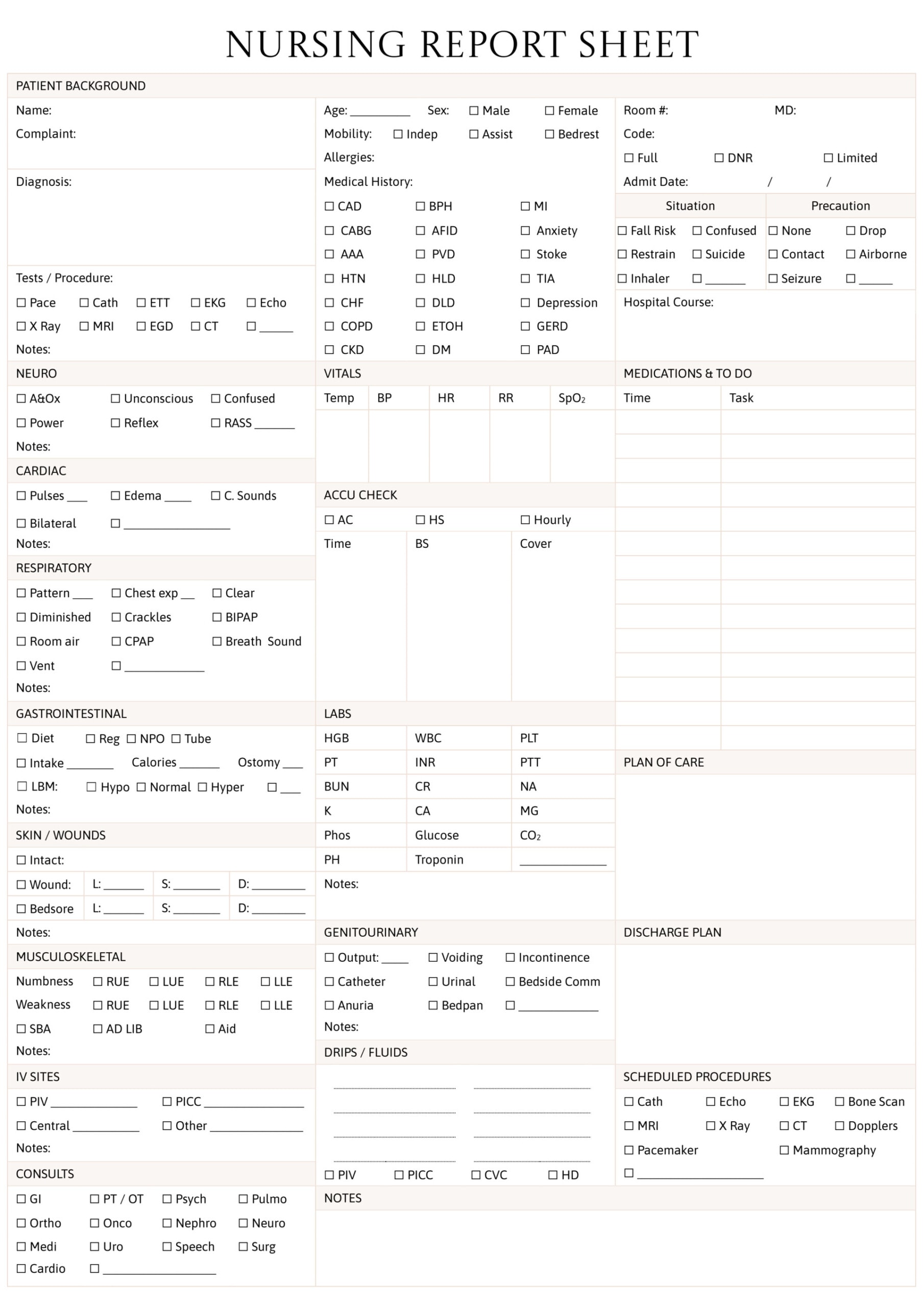
Patient Information
Use this section to document key patient details such as full name, room number, date of birth, age, gender, and admission date. These identifiers reduce the risk of errors like medication mix-ups or wrong-site procedures. You can also include the Patient ID for added safety, especially in large healthcare settings where patients may share similar names or details.
Allergies
Record known allergies or sensitivities to medications, foods, or materials. It’s recommended to ask the patient or their caregiver directly even if a chart is available. Accurate documentation can prevent serious reactions and keep patients safe.
Diagnosis
This section is used to document the patient’s current medical diagnosis or reason for admission, often called the nursing diagnosis. Include how the patient is responding to their condition and any related factors. Use clinical terms to help the next caregiver quickly understand the patient’s status and care priorities.
Vitals
Record the patient’s vital signs here, including pulse rate (PR), blood pressure (BP), respiratory rate (RR), and temperature (Temp). These readings should be updated consistently, as delays can lead to missed warning signs or complications.
Assessment
Clinical assessment involves observing and documenting the condition of key body systems including cardiovascular (CV), neurological (Neuro), genitourinary (GU), skin, blood glucose (BG), and lymph node status (NOD). It requires the nurse’s judgment to evaluate the patient’s physical and emotional condition. Irregularities such as abnormal heart rhythms, wounds, or swelling should be documented carefully. Comparing current findings with previous assessments can reveal meaningful changes and any unclear signs should be reported to attending physicians.
Medication
Document all medications the patient is currently receiving to prevent dosing errors and drug interactions. List each medication with the correct name, dose, route (e.g., oral, IV), and frequency. Note any missed doses or observed side effects. For high-alert medications like insulin, warfarin, morphine, and chemotherapy drugs, highlight them in the record using bold text or specific symbols for extra attention.
IV Therapy
Accurate IV documentation is important for managing fluid balance and timely medication delivery. Record the type of IV fluids, infusion rate, any additives, and the start time. You should also monitor the IV site regularly for signs of infiltration such as swelling, redness, or tenderness. If complications are observed, note the time, site location, and any steps taken to address the issue.
Laboratory Tests
Lab tests should be recorded with the test name and the date and time the sample was collected. Include important results when available to communicate critical findings to the medical team. Pending tests should also be noted so the next nurse can follow up appropriately.
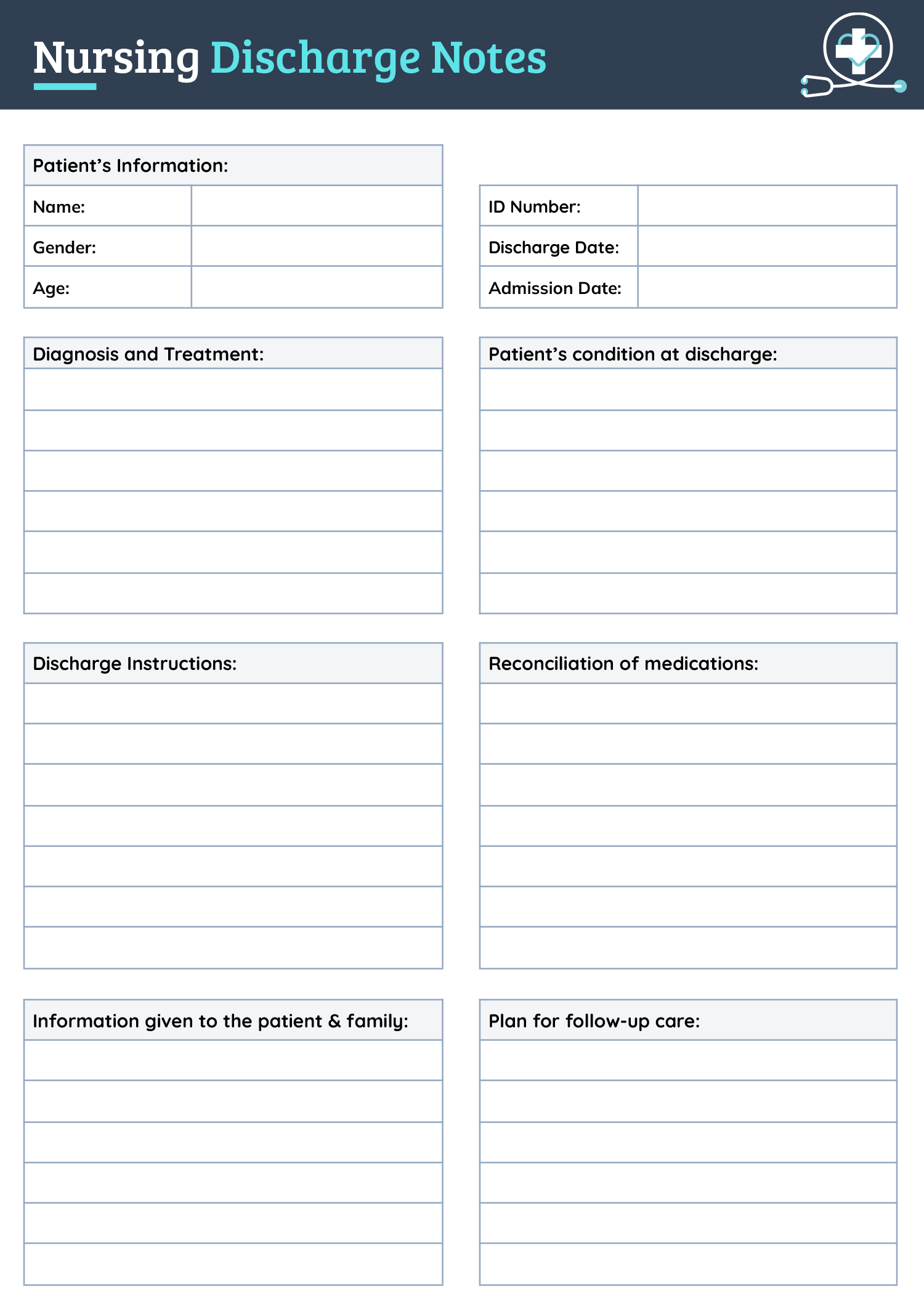
After double-checking all entries, sign the report, your signature confirms that you were present in the facility, provided care during the documented time, and are accountable for the information recorded. This signature also marks the report as complete and ready for transfer. Because these sheets serve as official medical records, always check for the previous nurse’s signature when receiving a report.